In practice I sometimes come across adults and children who suffer from a tongue tie. This relatively common affliction refers to the membranous structure underneath the tongue, called the frenulum linguae.

There is some suggestion that this structure shouldn’t be apparent at all. Embryologically the right and left sides of the tongue come together, fuse and then the tongue extends outwards during development. At this stage it is suggested the frenulum should recede completely. If it doesn’t, and it retains a degree of tension, this small structure has the capacity to effect an enormous number of issues in our lifetime.
A tongue tie is a poorly diagnosed and treated affliction. Mostly, it is never picked up and if so, reluctance to treat it is common. For the purposes of this article, it may be better to break down the issues in relation to what I find in a paediatric population compared to adults. Although the anatomy is similar, I commonly treat either group for entirely different symptomology.
The Anatomy
The tongue is a group of muscles (technically, it’s an organ) that have significant attachments and substantial fascial (also known as ‘connective tissue’, it supports and connects structures throughout the body, often forming networks that traverse large distances) planes. It attaches to bones in the throat (hyoid), the jaw (mandible) and the skull (temporal bone). The tongue has as much ability to affect any of these structures, as they have to affect the tongue.
The tongue is innervated by no less than 5 cranial (brain) nerves.
The tongue is involved in functions of speaking, swallowing, posture and alignment.
Children
Here I will outline some of the more common reasons that parents will bring their children to see me. Not all of these cases are related to tongue tie in that there are other potential causes, but tongue can can produce the following issues. When the mobility and therefore function of the tongue are affected, it won't be able to extend for long periods of time and may recoil (a possible cause of clicking when feeding) when the baby lowers the jaw during sucking. This results in breaking the seal and poor suction.
Sometimes there are problems breastfeeding. Some of the factors to consider include:
- Not latching on properly
- The latch cannot be sustained for long
- Sliding off the nipple
- Prolonged feeds
- Restlessness after prolonged feeds
- Falling asleep on the breast
- Gumming and chewing on the breast
- Not gaining weight
- Unable to utilise a dummy
Given the problems above, potential results that may ensue include:
- Nutritional deficits
- Colic
- Reflux
- Spilling from the side of the mouth
- Stimulation of the gag reflex
- Sleep apnoea
- Altered sleep patterns
- Speech problems
- Impairment of facial and jaw development
- Dental decay
- Teeth gapping
- The teeth either growing away from the tongue or inwards towards it
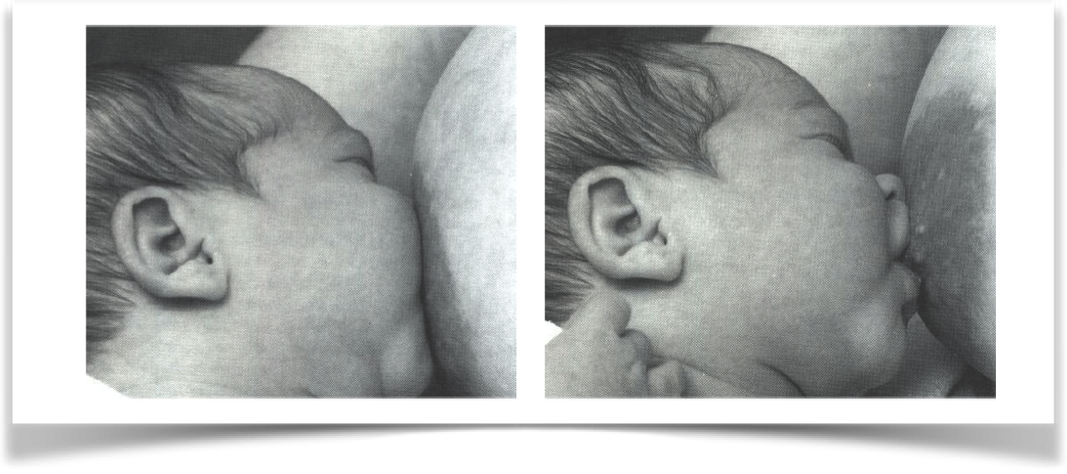
To breastfeed well and without pain requires a good and correct latch. This means:
- That the chin should rest on the breast, below the nipple
- The lips should roll outwards
- The lower lip (if not both) should be hinged outward
- The jaw is open wide (130-160 degrees)
- The top lip should be just above the nipple (not the areola)
Some of the more common issues from an improper latch include clicking noises from tongue recoil, colic and reflux.
If excessive amounts of air reach the stomach (Aerophagia) because of an improper swallow, the results can include:
- Abdominal distension
- Burping
- Flatulence
Colic (pain in the stomach or small intestine) usually produces crying and screaming and manifests within the first couple of weeks. It may last for several months. The exhaustion that comes from it can also be a reason why breastfeeding fails. Mothers are sometimes advised to wean but similar problems can also occur during bottle feeding.
Reflux can have colic type symptoms but usually involves regurgitation of milk or food. The pain and symptoms are usually worse on laying down flat, after feeding or when sleeping. It may result in the baby arching the back or neck to relieve the pain, coughing, gagging, drooling, problems swallowing and hiccoughing. The baby may refuse to feed (or conversely, constantly feed).
Unfortunately, treatment is often delayed to see if they symptoms will resolve themselves over
a few months. In a percentage of cases, infants may be placed on medications like Mylanta to reduce the reflux.
Is your child tongue tied?
If you were to sweep your finger across the floor of your child’s mouth, under the tongue, the floor should be smooth, which is great and indicates no problem. A small speed bump under the tongue may indicate a potential problem and a large speed bump will likely develop into issues. If you encounter a membrane under the tongue, problems are manifest.
The membrane itself may be very strong and feel like a piece of wire. If you push on it, look for a tongue tip indentation and bending of the tongue tip downwards.
The tongue tie will not correct of its own accord and will likely go on to affect breast feeding, breathing and speech - most likely the “l” and “th” sounds.
Treatment
If the problem is diagnosed and treated early enough, there should be minimal repercussions for the infant. Up until approximately 12 years of age, the bones of the face and cranium as still quite malleable. If the tensions created by the frenulum are allowed to exist over this period, the craniofacial development can be altered remarkably. There are many, many times I wish I had the chance to correct some adult issues when they were in childhood. In fact, the consequences in adulthood are so rampant that you could build a career out of treating them. I have written an article on adult tongue tie, which I would encourage you to read them as it provides different and more detailed information than I have written here.
Rather than treating the consequences, the most effective manual treatment will be no substitute for a frenectomy, This relatively simple procedure can be done in a dental practice with instruments or a laser. It doesn’t require a general anaesthetic (you can choose to have a local or nothing at all) or stitches. You will, however, have to adhere to an exercise program with your child for a couple of weeks so that the frenulum is prevented from scarring up.
 RSS Feed
RSS Feed