
Last week, the rollout of the SARS CoVid-2 vaccines began in Australia. Australia’s Prime Minister was amongst the first 20 to have the vaccine, calling it ‘a curtain raiser’ of what’s to come. Have you read the Vaccine program and bought your tickets yet?
There are many questions yet to be answered, and not just about the vaccine itself. The arguments for and against vaccination in the generalist sense are but one part in this play of many acts. Having paid our money, we should be wary of leaving after the first scene being told we have appreciated the whole drama.
If this play had been written 70 years ago, it may have been purely for the refreshment of its audience. Today, so many writers have had their contribution: medical, scientific, political, economic, government, and private enterprise and billionaires. So much so, that many have written themselves in as the main actors.
We live in times where we have been asked to accept the narrative, no questions asked. But the narrative is so complicated, nuanced and shrouded behind curtains of complicated, and often times, false and misleading data. Unless we are prepared to go to source information, to use scientific discernment of intricate and available research, follow the money trail and uncover the conflicts of interests and unethical and amoral actions of some of the players (which are a matter of public record), most of us will be content with the narrative in our play programs.
We have chosen to read this program because it doesn’t contain any questions and is only a few paragraphs of synopsis. There is a play next door that has a program with many questions, and has many thousands of pages of information about the performance and will take hundreds of hours to read. This play has very few patrons. Who will rise above human nature and who will invest the time and energy it takes to see it? The first play is relying on that to succeed.
This is a difficult piece to write when trying to focus solely on health aspects, for to understand why we must be asking questions it is necessary to appreciate the political and commercial aspects woven with the hegemonising, racketeering and whip handed approaches to this situation over a period of decades. To accept the current narrative is to consign, not just the autonomy over our own health, but our general freedoms to the shrinking pile of liberties. This is not who we are in this country.
The curtain must be drawn back and the wider stage appreciated here if we are to appreciate why this vaccine is not all about our health. It is not in the scope of this current article to elucidate further, but I would encourage you to spend 2 1/2 hours watching the following video:
Data Disaster: A Call for an Investigation Into the CDC’s Conduct During COVID-19
What kind of questions are pertinent to ask? To set the stage, they are not based around the historical story of ’to vaccinate or not to vaccinate’. They are based around the story of this particular vaccination. What is it? Is it safe? Has it undergone the necessary scientific rigour during testing? Is is designed to stop SARS CoVid 2 (CoVid19)? Is the Corona Virus data reliable? Is there a need to take it? How much of a threat is this particular virus? Are there any other alternatives? What does it mean for you if elderly and not in your 30’s? What does it mean for your newborn?
For example, the editorial in the British Medical Journal October 2020 was titled:
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us.
In the article, it was said:
The world has bet the farm on vaccines as the solution to the pandemic, but the trials are not focused on answering the questions many might assume they are. But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.
And, ...
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Then, ...
Yet the current phase III trials are not actually set up to prove either. None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
People have the right to form their own opinion about vaccines, both for and against. This is a premise from the medical fraternity itself who base their tenets on the work on Beauchamp and Childress who created the foundation of modern day bioethics. One of its four principles includes autonomy and enunciates: Autonomy requires the ability to decide for the self, free from control of the others, and with sufficient level of understanding so as to arrive at a meaningful choice. A person should have the capacity to decide upon a course of action, and to put that plan into action.
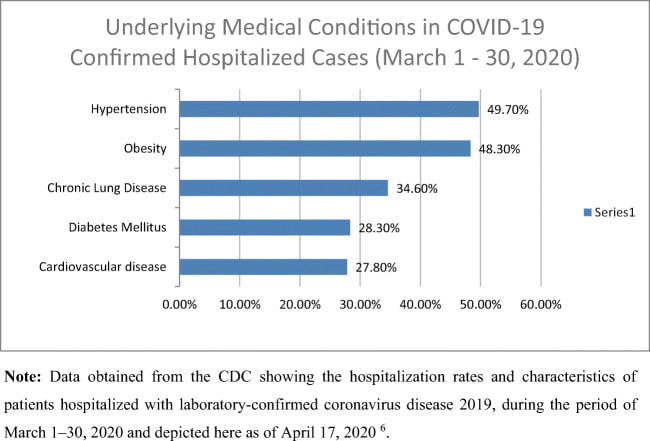
How then to reconcile the needs of the few with the many? In the case of SARS CoVid 2, which groups constitute the few, and which, the many? In the USA, one of the apparently hardest hit countries, the recovery rate (as of February 16, 2021) in the 0-64 age categories is 99.623%. In light of this does the virus necessitate mandatory or wide coverage vaccination?
Another of the four principles of bioethics details the notion of informed consent. If you are to undertake a procedure, you must do so in full knowledge of its possibilities and probabilities, potentials and pitfalls. Has this knowledge been disseminated, transparent and freely available, as it should? Are we even seeking it out?
What about the mortality rate? Taken at face value, the figures would suggest SARS CoVid 2 is more deadly than the flu. Staying with the USA, at the time of writing, the death toll is 498,993 according the the CDC. When you total the number of deaths against the number of positive cases (just shy of 28 million), it averages 1.73% of cases die with the virus.
At the start of the pandemic, the CDC changed the way it reported deaths with respect to corona virus. Why it did this ONLY for corona virus is a curious question? In short, if you die with the corona virus, despite several other co-morbid conditions, your cause of death is listed as the virus. Can it be proven that you died OF corona virus? No. Only that you died with it.
If the figures are tabulated according to the previous cause of death criteria, which seemed to serve fine for the previous 17 years, it turns out that corona virus deaths in the USA are 16.7 times LESS than today’s figures. This means the total death figure is closer to 29,880 unfortunate people.
How does this compare to the flu related deaths in the USA? During the 2019-2020 influenza season, CDC estimates that influenza was associated with 38 million illnesses, 18 million medical visits, 405,000 hospitalisations, and 22,000 deaths. These numbers are likely to grow. The CDC reports that results are still tabulated up to 2 years after the event.
Also note the overall burden of influenza for the 2017-2018 season was an estimated 45 million influenza illnesses, 21 million influenza-associated medical visits, 810,000 influenza-related hospitalisations, and 61,000 influenza-associated deaths.
Based on these numbers, how much of an emergency is SARS CoVid 2? It is because of this narrative that testing and trials have been pushed though at an alarming rate. On average, it would normally take 12 years to move a drug through trials to your bathroom cabinet. Ordinarily, 5 in 5000 drugs make it through approval to the first round of testing and only 1 in 5000 progresses to manufacture. The number approved drugs that are removed from use within the first few years is also alarming.
Normally, preclinical testing by the drug company is done on animals and in the lab to prove the drug works against the disease. It’s evaluated for safety and at no point is given to a human being. This phase takes typically takes 3 1/2 years.
Phase III trials are where the majority of adverse event testing is usually done, with questions based on side effects noticed in phase I and II trials. Generally, this takes around 3 years.
To date, there are nine vaccines being marketed having pushed through 6 stages of trials in the last 9-12 months. Questions need to be asked and answers with transparency must be given. The onus is now on us to do this because it is not being offered by the makers of the vaccines. Data is short and there have been NO independent tests of the procedures and outcomes by other, non-pharma company researchers. This is a normal requirement.
In short, we don’t know the medium to long term ramifications of these vaccines. According to rigorous scientific principles, claims made by pharmaceutical companies and governments (let alone owners of computer companies and social media outlets) about the safety and efficacy of these vaccines are not yet supported by empirical evidence. It is required of pharma companies and governments to do this. There is such a thing as duty of care and this can only be achieved if the vaccines are proven not to cause harm to the populous before they are implemented.
On the face of it, safety with these vaccines is presumed. It is not good enough to produce a retrospective study years down the track to assess and study safety after the fact. There is such a thing as the precautionary principle that places burden of proof on the makers and authorities rather than on the general public.
When proof of non-harm is placed upon the wider public, it is or can be used to protect the inherent interests of the pharmaceutical companies and those invested in vaccine development, rather than the people.
The takeaway message here is the underlying narrative of this situation and how it speaks to our health liberties now and in the future. In many ways the mainstream medical options are becoming narrower and more tightly controlled than ever before. There is some evidence to suggest the narrative it not what we have been told. As I alluded to in my last newsletter, we haven’t been talking enough about the general state of health in the world today as a springboard for CoVid-19 and many other wellness issues. There are things that everyone can do on the ground, now, today, naturally to promote health and avoid taking yet more medication and promote a highly effective immune system. There is more discussion to be had.
Be well.


 RSS Feed
RSS Feed