This post is a follow-on from the previous blog article on tongue-tie in children. It's worth reading as an adjunct to this article for adults ...
Because a tongue-tie in children is rarely treated, I see a lot of ankyloglossia in adults. By the time I see this in adult patients, years and decades of adaption have occurred. Therapists will very often and repeatedly treat the symptoms of a tongue-tie, for example, a degenerative neck, without addressing the causative circumstances.
Some of these secondary adaptions include:
Because a tongue-tie in children is rarely treated, I see a lot of ankyloglossia in adults. By the time I see this in adult patients, years and decades of adaption have occurred. Therapists will very often and repeatedly treat the symptoms of a tongue-tie, for example, a degenerative neck, without addressing the causative circumstances.
Some of these secondary adaptions include:
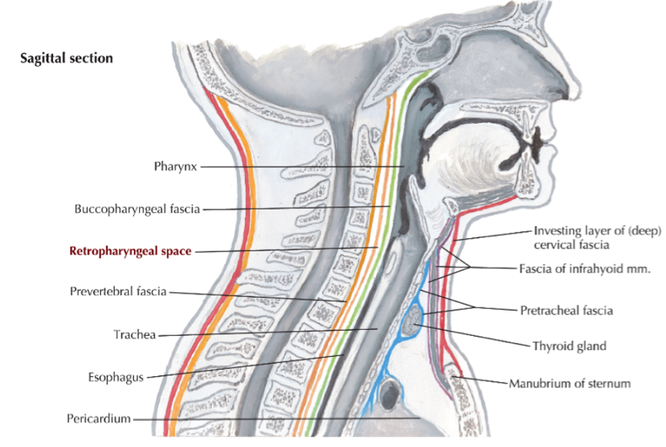
- An immobile sternum. Because of the fascial, muscular and neural connections from the mouth and jaw down to the sternal area, stiffness can result. This may lead to circumstances like altered breathing patterns, rib problems, lung and cardiac restrictions (due to sternopericadial and sternopleural attachments) and thoracic pain.
- Tightness around the base of the skull and upper neck, which may contribute to neck pain, headaches, swallowing issues …
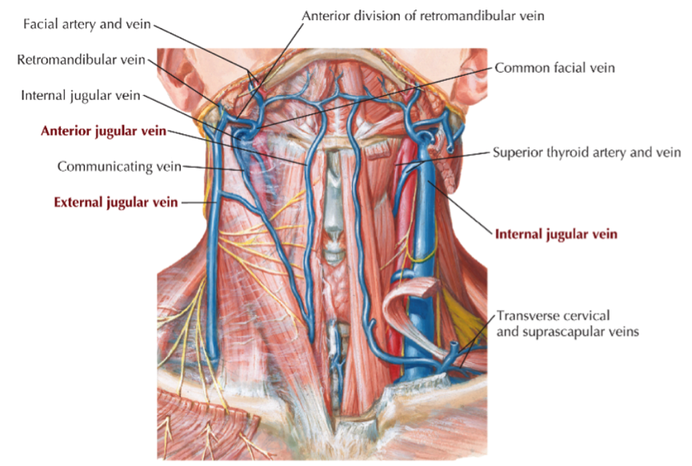
- Tension in the front of the neck or the muscles along the side of the neck. One side may be more tender than the other, which can link to a tighter frenulum on the same side.
- Tension in the bone and cartilage at the top of the throat. This should be fairly mobile to allow for correct speech and swallowing. It should easily move side to side and a restriction to one side may again correlate to a tighter frenulum on the side it has trouble moving away from.
- Tightness here may also pull the bone and cartilage upward which can translate tension all the way down to the stomach via the oesophagus. This is where reflux, heartburn and hiatial hernias can be apparent.
- Tightness in the muscles under the jaw. This can manifest as a straight line between the point of the chin and the throat, under the jaw. This can pull the jaw downwards and backwards, leading to TMJ issues.
- Tightness in the floor of the mouth. Any of my patients who’ve had mouth work done can tell you how tight these muscles can get. The tongue should be able to elevate towards the roof of the mouth without the floor of the mouth coming upwards.
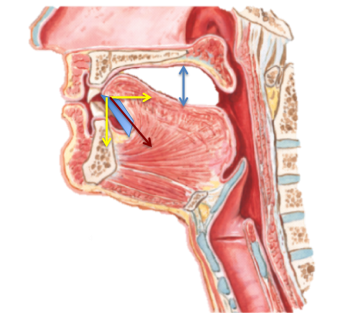
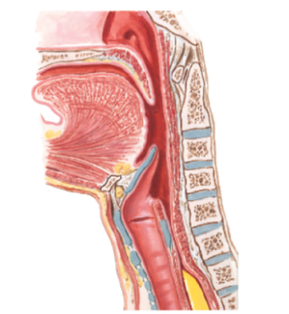
- At the same time, with a tight frenulum, often only the tip of the tongue will rest on the palate (behind the upper teeth). On the picture below left, the solid blue bar represents the frenulum; the red arrow represents the pull of the frenulum; the yellow vectors represent the resultant pull of the frenulum in the horizontal and vertical planes; the blue arrow is one of the eventual effects where the posterior tongue sits low and back, which produces an array of sucking, breathing, speech and TMJ problems. At rest, the middle and back parts of the tongue should nestle up against the back of the hard palate (picture on the right).
 |  |
- Tightness in the jaw muscles of the cheek. Ropey, sore muscles here may indicate that they are working too hard. A tight frenulum will cause the jaw to move backwards, disrupting the mechanics at the TMJ. This can also be a problem at night, as the same backwards movement can constrict the airways and contribute to an obstructive sleep apnoea.
- Tightness in other associated areas in the hands, arms, neck, back, sacrum, and pelvis.
- Speech and breathing issues. For example, mumbling and talking quietly or developing a sore throat or gravelly voice towards the end of the day. Also, it lends itself towards becoming a mouth breather, which leads to hyperventilation and poor diaphragm mechanics.
Good manual therapy can go a long way towards minimising or eliminating some or most of these issues. It will usually include a raft of home exercises, as well.
Some patients will opt for a frenectomy, which is a relatively quick procedure to release the membrane under the tongue, done in a dental practice experienced with this surgery. It is usually performed with a laser and doesn’t require anaesthetic. To prevent re-scarring, a month long regime of exercises is necessary. All surgery has potential complications, but should be minimal in this case and in the hands of a dentist who has some experience. Be careful of damage to the salivary glands under the tongue.
Post surgery, you might expect to feel or see:
- Better tongue movement
- More tongue relaxation
- A wider tongue
- The tongue sitting more on the roof of the mouth
- Better facial symmetry in the cheeks, nose, mouth or eyes
- Less grinding of the teeth
- Better sleep
- More relaxation and openness in the throat area
- Less chest tension
- Better neck and back posture
- Changes to a Dowager’s hump
- Less tension around the base of the skull
- Changes to ease of swallow
- Less back pain
This is a basic overview of some of the issues and possibilities surrounding a tight frenulum and therapy or surgery. Despite such a small restriction, the repercussions are manifest.

 RSS Feed
RSS Feed