Generally, I am moved to write an article when enough people present at the clinic with common symptoms relating to conditions that are poorly understood and not managed well in mainstream health.
Removal of the Gallbladder (Cholecystectomy) is one such condition, as are a number of possibly related conditions such as various types of reflux, anaemia, digestive issues, diarrhoea, vitamin deficiencies, osteoporosis and weight gain, just to name a small sample.
Removal of the Gallbladder (Cholecystectomy) is one such condition, as are a number of possibly related conditions such as various types of reflux, anaemia, digestive issues, diarrhoea, vitamin deficiencies, osteoporosis and weight gain, just to name a small sample.
Perusing the literature will reveal that somewhere between 7% and 47% (depending on the criteria) of patients are dissatisfied with the procedure. In some cases, that’s nearly half of the people who have this surgery! Of course the surgery is necessary in some cases (often in those who have left it too late to do something conservative about it) but questions have to be asked when a significant number of patients remain with the same complaints they experienced pre-surgery.
Duodenogastric reflux (DGR) is a normally occurring phenomenon whereby some of the pancreatic enzymes and bile delivered to the small intestine (the first part of which is called the duodenum) from the gallbladder leaks back up into the stomach. This normally doesn't produce any symptoms. However, leakage after cholecystectomy can occur at pathological levels. Studies show at least 20% and as much as 90% of patients demonstrate excessive DGR within 6 months of surgery.
At this point, note that Duodenogastric reflux (DGR) is different from Gastroesophageal Reflux (GOR) which occurs between the stomach and the oesophagus.
The problem with DGR in excessive amounts for prolonged periods is that it damages the protective stomach lining (mucosa) and can lead to inflammation or Bile Reflux Gastritis (BRG) and eventually, gastric ulcers.
At this juncture, two things can happen. An irritated stomach will go, at least partially, into spasm. This tension results in added stomach juices (a form of weak hydrochloric acid) being secreted from the stomach wall which can over-acidify the stomach, thus making the inflammation worse. Naturally, the stomach will want to get rid of it, so where does it go? Back up and out, which irritates the oesophagus.
The stomach is naturally on the acidic side and this helps to start the breakdown of food and also helps to kill of any unwanted bacteria that have snuck in. But, there is a balance: too much acid is irritating and too little (a tendency towards alkalinity) causes the stomach to somewhat delay the passage of food until it is broken down to the digestible levels. If it doesn’t do this, ‘undigested’ food is passed down the chain. The digestive process is specific to each part of the digestive chain and try as it might, the intestines may never catch up resulting in undigested food in the stool.
If the food does remain in the stomach too long, the partial fermentation that occurs feeds certain bacteria naturally present in the stomach and gut. The body is all about balance, and if certain bacteria start to dominate in the stomach, they can irritate the mucosa in the same fashion as already mentioned with the same result, or they can further imbalance the breakdown of food. This creates a negative cycle.
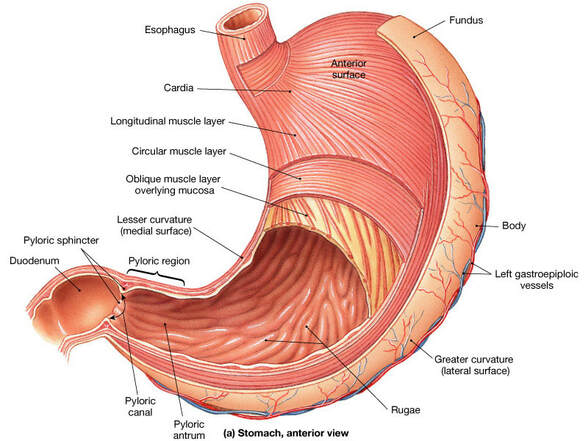
The second thing that can happen is when the alkaline bile and pancreatic juices back flow into the Antrum (see picture), the stomach then produces less somatostatin. Somatostatin helps to regulate the production of acid in the stomach. So when we eat, we produce more acid temporarily, but so we don’t produce too much, the stomach releases somatostatin to eventually shut down acid production. In effect, if the stomach becomes a little alkaline (due to duodenal reflux), somatostatin isn’t released in sufficient quantities and the net affect is that acid production continues to the point of hypersecretion and hyper-irritation of the inner stomach.
Statistically, if there were gallstones present, nearly 13% of patients are likely to develop a peptic ulcer within 5 years of surgery. This is only slightly more prevalent than those who had significant gallbladder irritation but didn’t have stones or surgical treatment. One way you could look at this is to say that for a number of people the problems that caused irritation remained, despite surgery. In fact, surgery in not aimed at a cure but only to remove the part that is causing pain. The precipitating circumstances remain and may then go on to affect other structures and functions with time.
Duodenogastric reflux (DGR) is a normally occurring phenomenon whereby some of the pancreatic enzymes and bile delivered to the small intestine (the first part of which is called the duodenum) from the gallbladder leaks back up into the stomach. This normally doesn't produce any symptoms. However, leakage after cholecystectomy can occur at pathological levels. Studies show at least 20% and as much as 90% of patients demonstrate excessive DGR within 6 months of surgery.
At this point, note that Duodenogastric reflux (DGR) is different from Gastroesophageal Reflux (GOR) which occurs between the stomach and the oesophagus.
The problem with DGR in excessive amounts for prolonged periods is that it damages the protective stomach lining (mucosa) and can lead to inflammation or Bile Reflux Gastritis (BRG) and eventually, gastric ulcers.
At this juncture, two things can happen. An irritated stomach will go, at least partially, into spasm. This tension results in added stomach juices (a form of weak hydrochloric acid) being secreted from the stomach wall which can over-acidify the stomach, thus making the inflammation worse. Naturally, the stomach will want to get rid of it, so where does it go? Back up and out, which irritates the oesophagus.
The stomach is naturally on the acidic side and this helps to start the breakdown of food and also helps to kill of any unwanted bacteria that have snuck in. But, there is a balance: too much acid is irritating and too little (a tendency towards alkalinity) causes the stomach to somewhat delay the passage of food until it is broken down to the digestible levels. If it doesn’t do this, ‘undigested’ food is passed down the chain. The digestive process is specific to each part of the digestive chain and try as it might, the intestines may never catch up resulting in undigested food in the stool.
If the food does remain in the stomach too long, the partial fermentation that occurs feeds certain bacteria naturally present in the stomach and gut. The body is all about balance, and if certain bacteria start to dominate in the stomach, they can irritate the mucosa in the same fashion as already mentioned with the same result, or they can further imbalance the breakdown of food. This creates a negative cycle.
The second thing that can happen is when the alkaline bile and pancreatic juices back flow into the Antrum (see picture), the stomach then produces less somatostatin. Somatostatin helps to regulate the production of acid in the stomach. So when we eat, we produce more acid temporarily, but so we don’t produce too much, the stomach releases somatostatin to eventually shut down acid production. In effect, if the stomach becomes a little alkaline (due to duodenal reflux), somatostatin isn’t released in sufficient quantities and the net affect is that acid production continues to the point of hypersecretion and hyper-irritation of the inner stomach.
Statistically, if there were gallstones present, nearly 13% of patients are likely to develop a peptic ulcer within 5 years of surgery. This is only slightly more prevalent than those who had significant gallbladder irritation but didn’t have stones or surgical treatment. One way you could look at this is to say that for a number of people the problems that caused irritation remained, despite surgery. In fact, surgery in not aimed at a cure but only to remove the part that is causing pain. The precipitating circumstances remain and may then go on to affect other structures and functions with time.
I see a skewed population of patients in the clinic on these terms. That is to say, I see the patients whose discomfort or dysfunction has remained despite surgery and I see it commonly enough to be moved to write this article. Figures show that 15%-20% of patients show with new gastrointestinal symptoms or the same preoperative complaints.
Further to the problems mentioned above, studies also show that antroduodenal (end of the stomach and beginning of the small intestine) motility is altered and stomach emptying is slowed following cholecystectomy. This may contribute to feelings of fullness, heaviness and distension discomfort following eating?
Other studies show that the healing and regeneration capabilities of the stomach mucosa are outpaced by the repeated stimulation of bile irritation due to DGR and may lead to chronic gastritis and metaplasia (growths, tumours, cysts, cancers, etc.) One researcher demonstrated that prolonged GDR longer than three years after gallbladder removal led to gastric pH exceeding 3 (strongly acidic) for prolonged periods and was associated with chronic gastritis.
Further to the problems mentioned above, studies also show that antroduodenal (end of the stomach and beginning of the small intestine) motility is altered and stomach emptying is slowed following cholecystectomy. This may contribute to feelings of fullness, heaviness and distension discomfort following eating?
Other studies show that the healing and regeneration capabilities of the stomach mucosa are outpaced by the repeated stimulation of bile irritation due to DGR and may lead to chronic gastritis and metaplasia (growths, tumours, cysts, cancers, etc.) One researcher demonstrated that prolonged GDR longer than three years after gallbladder removal led to gastric pH exceeding 3 (strongly acidic) for prolonged periods and was associated with chronic gastritis.
Another question that has to be asked is: with 10% to 15% of the population walking around with gallstones, why doesn’t everyone have problems? Gallstones don’t necessarily have to be the source of pain. Gallstones are associated with increased episodes of GDR but these don’t always correlate with symptoms.
Following surgery, removal of the gallbladder reservoir alters the cyclic pattern of bile excretion. It also alters the neurohumoral (a process whereby neural messages are altered to or from the organ due to a change in chemical stimuli, in this case, bile) response causing motility changes in the upper gastrointestinal tract, possibly leading to DGR.
One study performed an endoscopy of the oesophagus, stomach and duodenum 30 days prior to surgery and 60 days after surgery to determine the effects of the operation. The results were as follows:
1. In terms of inflammatory markers, 38% showed an increase pre-op and 48% post-op. More inflammation!
2. 38% had reduced activity / motility of the organs pre-op and post-op this increased to 64% of patients.
3. 34% had atrophy (breakdown) of the stomach lining prior to surgery and this increased to 48% post-op.
4. Intestinal metaplasia actually reduced from 46% pre-op to 44% post-op (but this still means 44% of people had some kind of metaplasia!)
5. 28% of patients demonstrated overly high levels of Helicobacter Pylori bacteria pre-op and this rose to 36% post-op.
Note: there will be more on H. Pylori bacteria to come in future articles.
Finally, in this article, it is important to note that discussion is centred around reflux occurring at the gastroduodenal junction (GDR) and not the gastrosophageal junction (GOR). The results at the GDR cannot be extrapolated to explain GOR.
Hopefully, this article gives you some background information on Gallbladder surgery and some of its effects. This should act as a springboard for further articles relating to associated dysfunctions, like osteoporosis and anaemia. Ultimately, this will also lead to a discussion on effective manual assessment and treatment options not generally considered by health providers.
Until then, good health.
Following surgery, removal of the gallbladder reservoir alters the cyclic pattern of bile excretion. It also alters the neurohumoral (a process whereby neural messages are altered to or from the organ due to a change in chemical stimuli, in this case, bile) response causing motility changes in the upper gastrointestinal tract, possibly leading to DGR.
One study performed an endoscopy of the oesophagus, stomach and duodenum 30 days prior to surgery and 60 days after surgery to determine the effects of the operation. The results were as follows:
1. In terms of inflammatory markers, 38% showed an increase pre-op and 48% post-op. More inflammation!
2. 38% had reduced activity / motility of the organs pre-op and post-op this increased to 64% of patients.
3. 34% had atrophy (breakdown) of the stomach lining prior to surgery and this increased to 48% post-op.
4. Intestinal metaplasia actually reduced from 46% pre-op to 44% post-op (but this still means 44% of people had some kind of metaplasia!)
5. 28% of patients demonstrated overly high levels of Helicobacter Pylori bacteria pre-op and this rose to 36% post-op.
Note: there will be more on H. Pylori bacteria to come in future articles.
Finally, in this article, it is important to note that discussion is centred around reflux occurring at the gastroduodenal junction (GDR) and not the gastrosophageal junction (GOR). The results at the GDR cannot be extrapolated to explain GOR.
Hopefully, this article gives you some background information on Gallbladder surgery and some of its effects. This should act as a springboard for further articles relating to associated dysfunctions, like osteoporosis and anaemia. Ultimately, this will also lead to a discussion on effective manual assessment and treatment options not generally considered by health providers.
Until then, good health.
 RSS Feed
RSS Feed